Medical cannabis
Cannabis sativa L. (marijuana; hemp) used medicinally
| Cannabis |
|---|
|
[[File:
 |200px|center|alt=]] |200px|center|alt=]]
|
Medical cannabis, medicinal cannabis or medical marijuana (MMJ) refers to cannabis products and cannabinoid molecules that are prescribed by physicians for their patients.<ref>,
Medicinal cannabis, Australian Prescriber, Vol. 38(Issue: 6), pp. 212–15, DOI: 10.18773/austprescr.2015.072, PMID: 26843715, PMC: 4674028,</ref><ref>
What is medical marijuana?(link). National Institute of Drug Abuse.
July 2015.
Accessed 19 April 2016.
</ref><ref>,
Medicinal cannabis for psychiatric disorders: a clinically-focused systematic review, BMC Psychiatry, Vol. 20(Issue: 1), DOI: 10.1186/s12888-019-2409-8, PMID: 31948424, PMC: 6966847,</ref><ref>O'Brien, Kylie, Medicinal Cannabis: Issues of evidence, European Journal of Integrative Medicine, Vol. 28, pp. 114–120, DOI: 10.1016/j.eujim.2019.05.009, Full text,</ref> The use of cannabis as medicine has a long history, but has not been as rigorously tested as other medicinal plants due to legal and governmental restrictions, resulting in limited clinical research to define the safety and efficacy of using cannabis to treat diseases.<ref>, Release the strains, Nature Medicine, Vol. 21(Issue: 9), DOI: 10.1038/nm.3946, PMID: 26340110,</ref>
Preliminary evidence has indicated that cannabis might reduce nausea and vomiting during chemotherapy and reduce chronic pain and muscle spasms.<ref name=Borgelt2013 /><ref name=JAMA2015 /> Regarding non-inhaled cannabis or cannabinoids, a 2021 review found that it provided little relief against chronic pain and sleep disturbance, and caused several transient adverse effects, such as cognitive impairment, nausea, and drowsiness.<ref name="wang2021">,
Medical cannabis or cannabinoids for chronic non-cancer and cancer related pain: a systematic review and meta-analysis of randomised clinical trials, BMJ, Vol. 374, pp. n1034, DOI: 10.1136/bmj.n1034, PMID: 34497047, Full text, Accessed on: 9 September 2021.</ref>
Short-term use increases the risk of minor and major adverse effects.<ref name=JAMA2015 /> Common side effects include dizziness, feeling tired, vomiting, and hallucinations.<ref name=JAMA2015 /> Long-term effects of cannabis are not clear.<ref name=JAMA2015 /> Concerns include memory and cognition problems, risk of addiction, schizophrenia in young people, and the risk of children taking it by accident.<ref name=Borgelt2013 />
Many cultures have used cannabis for therapeutic purposes for thousands of years.<ref name=BenAmar2006>,
Cannabinoids in medicine: A review of their therapeutic potential, Journal of Ethnopharmacology, Vol. 105(Issue: 1–2), pp. 1–25, DOI: 10.1016/j.jep.2006.02.001, PMID: 16540272,</ref> Some American medical organizations have requested removal of cannabis from the list of Schedule I controlled substances, emphasizing that rescheduling would enable more extensive research and regulatory oversight to ensure safe access.<ref name="ANA" /><ref name="AAFP" /> Others oppose its legalization, such as the American Academy of Pediatrics.<ref name="AAP" />
Medical cannabis can be administered through various methods, including capsules, lozenges, tinctures, dermal patches, oral or dermal sprays, cannabis edibles, and vaporizing or smoking dried buds. Synthetic cannabinoids are available for prescription use in some countries, such as synthetic delta-9-THC and nabilone.
Countries that allow the medical use of whole-plant cannabis include Argentina, Australia, Canada, Chile, Colombia, Germany, Greece, Israel, Italy, the Netherlands, Peru, Poland, Portugal, Spain, and Uruguay. In the United States, 38 states and the District of Columbia have legalized cannabis for medical purposes, beginning with the passage of California's Proposition 215 in 1996.<ref name="NCSL" /> Although cannabis remains prohibited for any use at the federal level, the Rohrabacher–Farr amendment was enacted in December 2014, limiting the ability of federal law to be enforced in states where medical cannabis has been legalized. This amendment reflects an increasing bipartisan acknowledgment of the potential therapeutic uses of cannabis and the significance of state-level policymaking in this area.
Classification
In the U.S., the National Institute on Drug Abuse defines medical cannabis as "using the whole, unprocessed marijuana plant or its basic extracts to treat symptoms of illness and other conditions".<ref name=nida>
Marijuana as Medicine(link). {{{website}}}. National Institute on Drug Abuse. July 2019.
Accessed 19 April 2016.
</ref>
A cannabis plant includes more than 400 different chemicals, of which about 70 are cannabinoids.<ref name="Consumer Reports April 2016">
Up in Smoke: Does Medical Marijuana Work?(link). Consumer Reports.
28 April 2016.
Accessed 24 May 2016.
</ref> In comparison, typical government-approved medications contain only one or two chemicals.<ref name="Consumer Reports April 2016" /> The number of active chemicals in cannabis is one reason why treatment with cannabis is difficult to classify and study.<ref name="Consumer Reports April 2016" />
A 2014 review stated that the variations in ratio of CBD-to-THC in botanical and pharmaceutical preparations determines the therapeutic vs psychoactive effects (CBD attenuates THC's psychoactive effects<ref name="Schubart et al.2014">,
Cannabidiol as a potential treatment for psychosis, European Neuropsychopharmacology, Vol. 24(Issue: 1), pp. 51–64, DOI: 10.1016/j.euroneuro.2013.11.002, PMID: 24309088, Full text, Accessed on: 9 July 2016.</ref>) of cannabis products.<ref name="ReferenceA">, Systematic review: efficacy and safety of medical marijuana in selected neurologic disorders: report of the Guideline Development Subcommittee of the American Academy of Neurology, Neurology, Vol. 82(Issue: 17), pp. 1556–1563, DOI: 10.1212/WNL.0000000000000363, PMID: 24778283, PMC: 4011465,</ref>
Medical uses
.jpg)
Overall, research into the health effects of medical cannabis has been of low quality and it is not clear whether it is a useful treatment for any condition, or whether harms outweigh any benefit.<ref name=pratt>,
Benefits and harms of medical cannabis: a scoping review of systematic reviews, Syst Rev, Vol. 8(Issue: 1), DOI: 10.1186/s13643-019-1243-x, PMID: 31823819, PMC: 6905063,</ref> There is no consistent evidence that it helps with chronic pain and muscle spasms.<ref name=pratt />
Low quality evidence suggests its use for reducing nausea during chemotherapy, improving appetite in HIV/AIDS, improving sleep, and improving tics in Tourette syndrome.<ref name=JAMA2015>,
Cannabinoids for Medical Use: A Systematic Review and Meta-analysis, JAMA, Vol. 313(Issue: 24), pp. 2456–73, DOI: 10.1001/jama.2015.6358, PMID: 26103030,</ref> When usual treatments are ineffective, cannabinoids have also been recommended for anorexia, arthritis, glaucoma,<ref name="Sachs et al. 2015" /> and migraine.<ref name="Distillations">
Sex(ism), Drugs, and Migraines: Distillations Podcast and Transcript, Episode 237(link). Distillations. Science History Institute. 15 January 2019.
Accessed 28 August 2019.
</ref>
It is unclear whether American states might be able to mitigate the adverse effects of the opioid epidemic by prescribing medical cannabis as an alternative pain management drug.<ref>,
The use of cannabis in response to the opioid crisis: A review of the literature, Nursing Outlook, Vol. 66(Issue: 1), pp. 56–65, DOI: 10.1016/j.outlook.2017.08.012, PMID: 28993073,</ref>
Cannabis should not be used in pregnancy.<ref>American College of Obstetricians Gynecologists Committee on Obstetric Practice,
Committee Opinion No. 637: Marijuana Use During Pregnancy and Lactation, Obstetrics and Gynecology, Vol. 126(Issue: 1), pp. 234–38, DOI: 10.1097/01.AOG.0000467192.89321.a6, PMID: 26241291,</ref>
Insomnia
Research analyzing data from the National Health and Nutrition Examination Survey (NHANES) did not find significant differences in sleep duration between cannabis users and non-users. This suggests that while some individuals may perceive benefits from cannabis use in terms of sleep, it may not significantly change overall sleep patterns across the general population.<ref>,
Recent cannabis use and nightly sleep duration in adults: a population analysis of the NHANES from 2005 to 2018, Regional Anesthesia & Pain Medicine, Vol. 47(Issue: 2), pp. 100–104, DOI: 10.1136/rapm-2021-103161, PMID: 34873024, Full text,</ref>
A review of literature up to 2018 indicates that cannabidiol (CBD) may have therapeutic potential for the treatment of insomnia. CBD, a non-psychoactive component of cannabis, is of particular interest due to its potential to influence sleep without the psychoactive effects associated with tetrahydrocannabinol (THC).<ref>,
Treating insomnia symptoms with medicinal cannabis: a randomized, crossover trial of the efficacy of a cannabinoid medicine compared with placebo, SLEEP, Vol. 44(Issue: 11), DOI: 10.1093/sleep/zsab149, PMID: 34115851, PMC: 8598183,</ref>
Nausea and vomiting
Medical cannabis is somewhat effective in chemotherapy-induced nausea and vomiting (CINV)<ref name=Borgelt2013 /><ref name="Sachs et al. 2015">,
Safety and Toxicology of Cannabinoids, Neurotherapeutics, Vol. 12(Issue: 4), pp. 735–46, DOI: 10.1007/s13311-015-0380-8, PMID: 26269228, PMC: 4604177,</ref> and may be a reasonable option in those who do not improve following preferential treatment.<ref name=Grotenhermen2012 /> Comparative studies have found cannabinoids to be more effective than some conventional antiemetics such as prochlorperazine, promethazine, and metoclopramide in controlling CINV,<ref name=Bowels2012>, The intersection between cannabis and cancer in the United States, Critical Reviews in Oncology/Hematology, Vol. 83(Issue: 1), pp. 1–10, DOI: 10.1016/j.critrevonc.2011.09.008, PMID: 22019199,</ref> but these are used less frequently because of side effects including dizziness, dysphoria, and hallucinations.<ref name=Wang2008>, Adverse effects of medical cannabinoids: a systematic review, CMAJ, Vol. 178(Issue: 13), pp. 1669–78, DOI: 10.1503/cmaj.071178, PMID: 18559804, PMC: 2413308,</ref><ref name=Jordan2007>, Guidelines for antiemetic treatment of chemotherapy-induced nausea and vomiting: past, present, and future recommendations, The Oncologist, Vol. 12(Issue: 9), pp. 1143–50, DOI: 10.1634/theoncologist.12-9-1143, PMID: 17914084, Full text,</ref> Long-term cannabis use may cause nausea and vomiting, a condition known as cannabinoid hyperemesis syndrome (CHS).<ref name=Nicolson2012>, Cannabinoid hyperemesis syndrome: a case series and review of previous reports, Psychosomatics, Vol. 53(Issue: 3), pp. 212–19, DOI: 10.1016/j.psym.2012.01.003, PMID: 22480624,</ref>
A 2016 Cochrane review said that cannabinoids were "probably effective" in treating chemotherapy-induced nausea in children, but with a high side-effect profile (mainly drowsiness, dizziness, altered moods, and increased appetite). Less common side effects were "ocular problems, orthostatic hypotension, muscle twitching, pruritus, vagueness, hallucinations, lightheadedness and dry mouth".<ref>,
Antiemetic medication for prevention and treatment of chemotherapy-induced nausea and vomiting in childhood, The Cochrane Database of Systematic Reviews, Vol. 2016(Issue: 2), pp. CD007786, DOI: 10.1002/14651858.CD007786.pub3, PMID: 26836199, PMC: 7073407, Full text, Accessed on: 23 September 2019.</ref>
HIV/AIDS
Evidence is lacking for both efficacy and safety of cannabis and cannabinoids in treating patients with HIV/AIDS or for anorexia associated with AIDS. As of 2013, current studies suffer from the effects of bias, small sample size, and lack of long-term data.<ref name=Lutge2013>,
The medical use of cannabis for reducing morbidity and mortality in patients with HIV/AIDS, The Cochrane Database of Systematic Reviews, Vol. 4(Issue: 4), pp. CD005175, DOI: 10.1002/14651858.CD005175.pub3, PMID: 23633327,</ref>
Pain
A 2021 review found little effect of using non-inhaled cannabis to relieve chronic pain.<ref name=wang2021/> According to a 2019 systematic review, there have been inconsistent results of using cannabis for neuropathic pain, spasms associated with multiple sclerosis and pain from rheumatic disorders, but was not effective treating chronic cancer pain. The authors state that additional randomized controlled trials of different cannabis products are necessary to make conclusive recommendations.<ref name=pratt/>
When cannabis is inhaled to relieve pain, blood levels of cannabinoids rise faster than when oral products are used, peaking within three minutes and attaining an analgesic effect in seven minutes.<ref name="aviram">,
Efficacy of Cannabis-Based Medicines for Pain Management: A Systematic Review and Meta-Analysis of Randomized Controlled Trials, Pain Physician, Vol. 20(Issue: 6), pp. E755–96, DOI: 10.36076/ppj.20.5.E755, PMID: 28934780, Full text, Accessed on: 12 January 2018.</ref>
A 2011 review considered cannabis to be generally safe,<ref name=Lyn2011>,
Cannabinoids for treatment of chronic non-cancer pain; a systematic review of randomized trials, British Journal of Clinical Pharmacology, Vol. 72(Issue: 5), pp. 735–44, DOI: 10.1111/j.1365-2125.2011.03970.x, PMID: 21426373, PMC: 3243008,</ref> and it appears safer than opioids in palliative care.<ref name=Carter2011>, Cannabis in palliative medicine: improving care and reducing opioid-related morbidity, The American Journal of Hospice & Palliative Care, Vol. 28(Issue: 5), pp. 297–303, DOI: 10.1177/1049909111402318, PMID: 21444324,</ref>
A 2022 review concluded the pain relief experienced after using medical cannabis is due to the placebo effect, especially given widespread media attention that sets the expectation for pain relief.<ref>,
Placebo Response and Media Attention in Randomized Clinical Trials Assessing Cannabis-Based Therapies for PainA Systematic Review and Meta-analysis, JAMA Network Open, Vol. 5(Issue: 11), pp. e2243848, DOI: 10.1001/jamanetworkopen.2022.43848, PMID: 36441553, PMC: 9706362,</ref>
Neurological conditions
Cannabis' efficacy is not clear in treating neurological problems, including multiple sclerosis (MS) and movement problems.<ref name="ReferenceA"/> Evidence also suggests that oral cannabis extract is effective for reducing patient-centered measures of spasticity.<ref name="ReferenceA"/> A trial of cannabis is deemed to be a reasonable option if other treatments have not been effective.<ref name=Borgelt2013 /> [by whom?]
Its use for MS is approved in ten countries.<ref name=Borgelt2013 /><ref name=Clark2011>, Medical marijuana: medical necessity versus political agenda, Medical Science Monitor, Vol. 17(Issue: 12), pp. RA249–61, DOI: 10.12659/MSM.882116, PMID: 22129912, PMC: 3628147,</ref>Template:COI source A 2012 review found no problems with tolerance, abuse, or addiction.<ref>, [Treatment of spasticity in multiple sclerosis: new perspectives regarding the use of cannabinoids], Revista de Neurología, Vol. 55(Issue: 7), pp. 421–30, PMID: 23011861,</ref> In the United States, cannabidiol, one of the cannabinoids found in the marijuana plant, has been approved for treating two severe forms of epilepsy, Lennox-Gastaut syndrome and Dravet syndrome.<ref name=":4">Commissioner, Office of the, FDA and Marijuana, FDA, Full text, Accessed on: 16 December 2019.</ref>
Mental health
A 2019 systematic review found that there is a lack of evidence that cannabinoids are effective in treating depressive or anxiety disorders, attention-deficit hyperactivity disorder (ADHD), Tourette syndrome, post-traumatic stress disorder, or psychosis.<ref name=black>,
Cannabinoids for the treatment of mental disorders and symptoms of mental disorders: a systematic review and meta-analysis, Lancet Psychiatry, Vol. 6(Issue: 12), pp. 995–1010, DOI: 10.1016/S2215-0366(19)30401-8, PMID: 31672337, PMC: 6949116,</ref>
Research indicates that cannabis, particularly CBD, may have anxiolytic (anxiety-reducing) effects. A study found that CBD significantly reduced anxiety during a simulated public speaking test for individuals with social anxiety disorder. However, the relationship between cannabis use and anxiety symptoms is complex, and while some users report relief, the overall evidence from observational studies and clinical trials remains inconclusive. Cannabis is often used by people to cope with anxiety, yet the efficacy and safety of cannabis for treating anxiety disorders is yet to be researched.<ref>
Anxiety and Cannabis: A Review of Recent Research(link). Medical Cannabis Research Center.
2023-04-10.
Accessed 2024-04-09.
</ref><ref>,
Medicinal cannabis for psychiatric disorders: a clinically-focused systematic review, BMC Psychiatry, Vol. 20(Issue: 1), DOI: 10.1186/s12888-019-2409-8, PMID: 31948424, PMC: 6966847,</ref>
Cannabis use, especially at high doses, is associated with a higher risk of psychosis, particularly in individuals with a genetic predisposition to psychotic disorders like schizophrenia. Some studies have shown that cannabis can trigger a temporary psychotic episode, which may increase the risk of developing a psychotic disorder later.<ref name=":5"> Abuse, National Institute on Drug. Is there a link between marijuana use and psychiatric disorders? | National Institute on Drug Abuse (NIDA)(link). nida.nih.gov.
2023-05-08.
Accessed 2024-04-09.
</ref>
The impact of cannabis on depression is less clear. Some studies suggest a potential increase in depression risk among adolescents who use cannabis, though findings are inconsistent across studies.<ref name=":5" />
Adverse effects
.jpg)
Medical use
There is insufficient data to draw strong conclusions about the safety of medical cannabis.<ref name=oxpain>,
Pain, Oxford University Press, 2012, ISBN 978-0-19-994274-9,</ref> Typically, adverse effects of medical cannabis use are not serious;<ref name=Borgelt2013>, The pharmacologic and clinical effects of medical cannabis, Pharmacotherapy, Vol. 33(Issue: 2), pp. 195–209, DOI: 10.1002/phar.1187, PMID: 23386598, Full text, Accessed on: 11 November 2017.</ref> they include tiredness, dizziness, increased appetite, and cardiovascular and psychoactive effects. Other effects can include impaired short-term memory; impaired motor coordination; altered judgment; and paranoia or psychosis at high doses.<ref>, Association Between Cannabis and Psychosis: Epidemiologic Evidence, Biological Psychiatry, Vol. 79(Issue: 7), pp. 549–56, DOI: 10.1016/j.biopsych.2015.08.001, PMID: 26386480, Full text, Accessed on: 11 March 2020.</ref> Tolerance to these effects develops over a period of days or weeks. The amount of cannabis normally used for medicinal purposes is not believed to cause any permanent cognitive impairment in adults, though long-term treatment in adolescents should be weighed carefully as they are more susceptible to these impairments. Withdrawal symptoms are rarely a problem with controlled medical administration of cannabinoids. The ability to drive vehicles or to operate machinery may be impaired until a tolerance is developed.<ref name=Grotenhermen2012>, The therapeutic potential of cannabis and cannabinoids, Deutsches Ärzteblatt International, Vol. 109(Issue: 29–30), pp. 495–501, DOI: 10.3238/arztebl.2012.0495, PMID: 23008748, PMC: 3442177,</ref> Although supporters of medical cannabis say that it is safe,<ref name=oxpain /> further research is required to assess the long-term safety of its use.<ref name=Wang2008 /><ref name=barceloux866931>Donald G, Medical Toxicology of Drug Abuse: Synthesized Chemicals and Psychoactive Plants, John Wiley & Sons, 2012, ISBN 978-0-471-72760-6, Accessed: 20 December 2015. Pages: 886–931,</ref>
Cognitive effects
Recreational use of cannabis is associated with cognitive deficits, especially for those who begin to use cannabis in adolescence. As of 2021[update] there is a lack of research into long-term cognitive effects of medical use of cannabis, but one 12-month observational study reported that "MC patients demonstrated significant improvements on measures of executive function and clinical state over the course of 12 months".<ref>,
An Observational, Longitudinal Study of Cognition in Medical Cannabis Patients over the Course of 12 Months of Treatment: Preliminary Results, Journal of the International Neuropsychological Society, Vol. 27(Issue: 6), pp. 648–60, DOI: 10.1017/S1355617721000114, PMID: 34261553,</ref>
Impact on psychosis
Exposure to THC can cause acute transient psychotic symptoms in healthy individuals and people with schizophrenia.<ref name="Schubart et al.2014" />
A 2007 meta analysis concluded that cannabis use reduced the average age of onset of psychosis by 2.7 years relative to non-cannabis use.<ref>,
Cannabis use and earlier onset of psychosis: a systematic meta-analysis, Archives of General Psychiatry, Vol. 68(Issue: 6), pp. 555–61, DOI: 10.1001/archgenpsychiatry.2011.5, PMID: 21300939,</ref> A 2005 meta analysis concluded that adolescent use of cannabis increases the risk of psychosis, and that the risk is dose-related.<ref>, Cannabis as a risk factor for psychosis: systematic review, Journal of Psychopharmacology, Vol. 19(Issue: 2), pp. 187–94, DOI: 10.1177/0269881105049040, PMID: 15871146,</ref> A 2004 literature review on the subject concluded that cannabis use is associated with a two-fold increase in the risk of psychosis, but that cannabis use is "neither necessary nor sufficient" to cause psychosis.<ref name=Arseneault2004>, Causal association between cannabis and psychosis: examination of the evidence, The British Journal of Psychiatry, Vol. 184(Issue: 2), pp. 110–17, DOI: 10.1192/bjp.184.2.110, PMID: 14754822,</ref> A French review from 2009 came to a conclusion that cannabis use, particularly that before age 15, was a factor in the development of schizophrenic disorders.<ref name="Laqueille">, [Is cannabis a vulnerability factor in schizophrenic disorders], Archives de Pédiatrie, Vol. 16(Issue: 9), pp. 1302–05, DOI: 10.1016/j.arcped.2009.03.016, PMID: 19640690,</ref>
Pharmacology
The genus Cannabis contains two species which produce useful amounts of psychoactive cannabinoids: Cannabis indica and Cannabis sativa, which are listed as Schedule I medicinal plants in the US;<ref name=Borgelt2013 /> a third species, Cannabis ruderalis, has few psychogenic properties.<ref name=Borgelt2013 /> Cannabis contains more than 460 compounds;<ref name=BenAmar2006 /> at least 80 of these are cannabinoids<ref>,
Phytocannabinoids, CNS cells and development: a dead issue?, Drug and Alcohol Review, Vol. 29(Issue: 1), pp. 91–98, DOI: 10.1111/j.1465-3362.2009.00102.x, PMID: 20078688,</ref><ref>, Cannabinoid analgesia as a potential new therapeutic option in the treatment of chronic pain, The Annals of Pharmacotherapy, Vol. 40(Issue: 2), pp. 251–60, DOI: 10.1345/aph.1G217, PMID: 16449552,</ref> – chemical compounds that interact with cannabinoid receptors in the brain.<ref name=Borgelt2013 /> As of 2012, more than 20 cannabinoids were being studied by the U.S. FDA.<ref name=Svrakic2012>, Legalization, decriminalization & medicinal use of cannabis: a scientific and public health perspective, Missouri Medicine, 2012, Vol. 109(Issue: 2), pp. 90–98, PMID: 22675784, PMC: 6181739,</ref>
The most psychoactive cannabinoid found in the cannabis plant is tetrahydrocannabinol (or delta-9-tetrahydrocannabinol, commonly known as THC).<ref name=BenAmar2006 /> Other cannabinoids include delta-8-tetrahydrocannabinol, cannabidiol (CBD), cannabinol (CBN), cannabicyclol (CBL), cannabichromene (CBC) and cannabigerol (CBG); they have less psychotropic effects than THC, but may play a role in the overall effect of cannabis.<ref name=BenAmar2006 /> The most studied are THC, CBD and CBN.<ref name=Gordon2013>,
Medical consequences of marijuana use: a review of current literature, Current Psychiatry Reports, Vol. 15(Issue: 12), DOI: 10.1007/s11920-013-0419-7, PMID: 24234874, Full text, Accessed on: 12 July 2019.</ref>
CB1 and CB2 are the primary cannabinoid receptors responsible for several of the effects of cannabinoids, although other receptors may play a role as well. Both belong to a group of receptors called G protein-coupled receptors (GPCRs). CB1 receptors are found in very high levels in the brain and are thought to be responsible for psychoactive effects.<ref>,
Cannabinoid receptors: where they are and what they do, Journal of Neuroendocrinology, Vol. 20(Issue: Suppl 1), pp. 10–14, DOI: 10.1111/j.1365-2826.2008.01671.x, PMID: 18426493,</ref> CB2 receptors are found peripherally throughout the body and are thought to modulate pain and inflammation.<ref>, The role of the cannabinoid CB2 receptor in pain transmission and therapeutic potential of small molecule CB2 receptor agonists, Current Medicinal Chemistry, Vol. 14(Issue: 8), pp. 917–36, DOI: 10.2174/092986707780363023, PMID: 17430144,</ref>
Absorption
Cannabinoid absorption is dependent on its route of administration.
Inhaled and vaporized THC have similar absorption profiles to smoked THC, with a bioavailability ranging from 10 to 35%. Oral administration has the lowest bioavailability of approximately 6%, variable absorption depending on the vehicle used, and the longest time to peak plasma levels (2 to 6 hours) compared to smoked or vaporized THC.<ref name=":0">,
Pharmacology of cannabinoids in the treatment of epilepsy, Epilepsy & Behavior, Vol. 70(Issue: Pt B), pp. 313–18, DOI: 10.1016/j.yebeh.2016.11.016, PMID: 28087250,</ref>
Similar to THC, CBD has poor oral bioavailability, approximately 6%. The low bioavailability is largely attributed to significant first-pass metabolism in the liver and erratic absorption from the gastrointestinal tract. However, oral administration of CBD has a faster time to peak concentrations (2 hours) than THC.<ref name=":0" />
Due to the poor bioavailability of oral preparations, alternative routes of administration have been studied, including sublingual and rectal. These alternative formulations maximize bioavailability and reduce first-pass metabolism. Sublingual administration in rabbits yielded bioavailability of 16% and time to peak concentration of 4 hours.<ref>,
Sublingual administration of Delta9-tetrahydrocannabinol/beta-cyclodextrin complex increases the bioavailability of Delta9-tetrahydrocannabinol in rabbits, Life Sciences, Vol. 78(Issue: 17), pp. 1911–14, DOI: 10.1016/j.lfs.2005.08.025, PMID: 16266727,</ref> Rectal administration in monkeys doubled bioavailability to 13.5% and achieved peak blood concentrations within 1 to 8 hours after administration.<ref name=":1">, Human cannabinoid pharmacokinetics, Chemistry & Biodiversity, Vol. 4(Issue: 8), pp. 1770–804, DOI: 10.1002/cbdv.200790152, PMID: 17712819, PMC: 2689518,</ref>
Distribution
Like cannabinoid absorption, distribution is also dependent on route of administration. Smoking and inhalation of vaporized cannabis have better absorption than do other routes of administration, and therefore also have more predictable distribution.<ref name=":1" /><ref name=":3">,
A review of oral cannabinoids and medical marijuana for the treatment of chemotherapy-induced nausea and vomiting: a focus on pharmacokinetic variability and pharmacodynamics, Cancer Chemotherapy and Pharmacology, Vol. 80(Issue: 3), pp. 441–49, DOI: 10.1007/s00280-017-3387-5, PMID: 28780725, PMC: 5573753,</ref> THC is highly protein bound once absorbed, with only 3% found unbound in the plasma. It distributes rapidly to highly vascularized organs such as the heart, lungs, liver, spleen, and kidneys, as well as to various glands. Low levels can be detected in the brain, testes, and unborn fetuses, all of which are protected from systemic circulation via barriers.<ref>, The pharmacokinetics of THC in fat and brain: resulting functional responses to marihuana smoking, Human Psychopharmacology, Vol. 16(Issue: 3), pp. 247–55, DOI: 10.1002/hup.258, PMID: 12404577,</ref> THC further distributes into fatty tissues a few days after administration due to its high lipophilicity, and is found deposited in the spleen and fat after redistribution.<ref name=":3" /><ref>, Medicinal Cannabis: History, Pharmacology, And Implications for the Acute Care Setting, P & T, Vol. 42(Issue: 3), pp. 180–88, PMID: 28250701, PMC: 5312634,</ref><ref>, Marihuana and Medicine. online version, Springer Science & Business Media, 1999, ISBN 978-1-59259-710-9, Accessed: 20 September 2020.</ref>
Metabolism
Delta-9-THC is the primary molecule responsible for the effects of cannabis. Delta-9-THC is metabolized in the liver and turns into 11-OH-THC.<ref name=":2"> ,
Human Metabolism of THC Full text, Sapiensoup Blog, 2016-12-21, Accessed on: 2017-11-01.
</ref> 11-OH-THC is the first metabolic product in this pathway. Both Delta-9-THC and 11-OH-THC are psychoactive. The metabolism of THC into 11-OH-THC plays a part in the heightened psychoactive effects of edible cannabis.<ref>
11-Hydroxy-THC - Increased Potency That Explains the Effect of Edibles? – Prof of Pot(link). profofpot.com.
2 July 2016.
Accessed 2017-11-01.
</ref>
Next, 11-OH-THC is metabolized in the liver into 11-COOH-THC, which is the second metabolic product of THC.<ref>
Toxicology Litigation Support: Marijuana(link). consultox.com.
Accessed 2017-11-01.
</ref> 11-COOH-THC is not psychoactive.<ref name=":2" />
Ingestion of edible cannabis products lead to a slower onset of effect than the inhalation of it because the THC travels to the liver first through the blood before it travels to the rest of the body. Inhaled cannabis can result in THC going directly to the brain, where it then travels from the brain back to the liver in recirculation for metabolism.<ref name=":2" /> Eventually, both routes of metabolism result in the metabolism of psychoactive THC to inactive 11-COOH-THC.
Excretion
Due to substantial metabolism of THC and CBD, their metabolites are excreted mostly via feces, rather than by urine.<ref name=":0" /><ref name="devinsky">,
Cannabidiol: pharmacology and potential therapeutic role in epilepsy and other neuropsychiatric disorders, Epilepsia, Vol. 55(Issue: 6), pp. 791–802, DOI: 10.1111/epi.12631, PMID: 24854329, PMC: 4707667,</ref> After delta-9-THC is hydroxylated into 11-OH-THC via CYP2C9, CYP2C19, and CYP3A4, it undergoes phase II metabolism into more than 30 metabolites, a majority of which are products of glucuronidation. Approximately 65% of THC is excreted in feces and 25% in the urine, while the remaining 10% is excreted by other means.<ref name=":0" /> The terminal half-life of THC is 25 to 36 hours,<ref>, Pharmacokinetics and pharmacodynamics of cannabinoids, Clinical Pharmacokinetics, Vol. 42(Issue: 4), pp. 327–60, DOI: 10.2165/00003088-200342040-00003, PMID: 12648025,</ref> whereas for CBD it is 18 to 32 hours.<ref name=devinsky/>
CBD is hydroxylated by P450 liver enzymes into 7-OH-CBD. Its metabolites are products of primarily CYP2C19 and CYP3A4 activity, with potential activity of CYP1A1, CYP1A2, CYP2C9, and CYP2D6.<ref>,
Cannabinoids and Cytochrome P450 Interactions, Current Drug Metabolism, Vol. 17(Issue: 3), pp. 206–226, DOI: 10.2174/1389200217666151210142051, PMID: 26651971, Full text, Accessed on: 1 November 2017.</ref> Similar to delta-9-THC, a majority of CBD is excreted in feces and some in the urine.<ref name=":0" /> The terminal half-life is approximately 18–32 hours.<ref>, Single-dose kinetics of deuterium-labelled cannabidiol in man after smoking and intravenous administration, Biomedical & Environmental Mass Spectrometry, Vol. 13(Issue: 2), pp. 77–83, DOI: 10.1002/bms.1200130206, PMID: 2937482,</ref>
Administration

Smoking has been the means of administration of cannabis for many users, but it is not suitable for the use of cannabis as a medicine.<ref name=CurtisClarke2009>,
Cannabinoids for Tourette's Syndrome, The Cochrane Database of Systematic Reviews, Vol. 2009(Issue: 4), pp. CD006565, DOI: 10.1002/14651858.CD006565.pub2, PMID: 19821373, PMC: 7387115,</ref> It was the most common method of medical cannabis consumption in the US as of 2013[update].<ref name=Borgelt2013 /> It is difficult to predict the pharmacological response to cannabis because concentration of cannabinoids varies widely, as there are different ways of preparing it for consumption (smoked, applied as oils, eaten, infused into other foods, or drunk) and a lack of production controls.<ref name=Borgelt2013 /> The potential for adverse effects from smoke inhalation makes smoking a less viable option than oral preparations.<ref name=CurtisClarke2009 /> Cannabis vaporizers have gained popularity because of a perception among users that fewer harmful chemicals are ingested when components are inhaled via aerosol rather than smoke.<ref name=Borgelt2013 /> Cannabinoid medicines are available in pill form (dronabinol and nabilone) and liquid extracts formulated into an oromucosal spray (nabiximols).<ref name=Borgelt2013 /> Oral preparations are "problematic due to the uptake of cannabinoids into fatty tissue, from which they are released slowly, and the significant first-pass liver metabolism, which breaks down Δ9THC and contributes further to the variability of plasma concentrations".<ref name=CurtisClarke2009 />
The US Food and Drug Administration (FDA) has not approved smoked cannabis for any condition or disease, as it deems that evidence is lacking concerning safety and efficacy.<ref name=FDA2006 /> The FDA issued a 2006 advisory against smoked medical cannabis stating: "marijuana has a high potential for abuse, has no currently accepted medical use in treatment in the United States, and has a lack of accepted safety for use under medical supervision."<ref name=FDA2006> </ref>
History
Ancient
Cannabis, called má 麻 (meaning "hemp; cannabis; numbness") or dàmá 大麻 (with "big; great") in Chinese, was used in Taiwan for fiber starting about 10,000 years ago.<ref>Ernest L.,
Marihuana: the first twelve thousand years, New York City:Plenum Publishers, 1980, ISBN 978-0-306-40496-2, Accessed: 29 October 2008.
[page needed]</ref> The botanist Hui-lin Li wrote that in China, "The use of Cannabis in medicine was probably a very early development. Since ancient humans used hemp seed as food, it was quite natural for them to also discover the medicinal properties of the plant."<ref>Li, Hui-Lin (1974). "An Archaeological and Historical Account of Cannabis in China", Economic Botany 28.4:437–48, p. 444.</ref> Emperor Shen-Nung, who was also a pharmacologist, wrote a book on treatment methods in 2737 BCE that included the medical benefits of cannabis. He recommended the substance for many ailments, including constipation, gout, rheumatism, and absent-mindedness.<ref name=autogenerated2>Edward,
Marijuana: The Second Trip, California:Glencoe Press, 1971,</ref> Cannabis is one of the 50 "fundamental" herbs in traditional Chinese medicine.<ref name="Wong">Ming, La Médecine chinoise par les plantes, Paris:Tchou, 1976,
[page needed]</ref>
The Ebers Papyrus (c. 1550 BCE) from Ancient Egypt describes medical cannabis.<ref name="ebers">Template:Unreliable source?
The Ebers Papyrus The Oldest (confirmed) Written Prescriptions For Medical Marihuana era 1,550 BC(link). {{{website}}}. onlinepot.org.
Accessed 10 June 2008.
</ref> The ancient Egyptians used hemp (cannabis) in suppositories for relieving the pain of hemorrhoids.<ref>
Pain, Stephanie,
The Pharaoh's pharmacists Full text, New Scientist, Reed Business Information Ltd., 15 December 2007, Accessed on: 4 September 2017.
</ref>
Surviving texts from ancient India confirm that cannabis' psychoactive properties were recognized, and doctors used it for treating a variety of illnesses and ailments, including insomnia, headaches, gastrointestinal disorders, and pain, including during childbirth.<ref>,
The religious and medicinal uses of Cannabis in China, India and Tibet, Journal of Psychoactive Drugs, 1981, Vol. 13(Issue: 1), pp. 23–34, DOI: 10.1080/02791072.1981.10471447, PMID: 7024492,</ref>
The Ancient Greeks used cannabis to dress wounds and sores on their horses,<ref name="hawthorne">,
The Medical Use of Cannabis Among the Greeks and Romans, Journal of Cannabis Therapeutics, 2002, Vol. 2(Issue: 2), pp. 51–70, DOI: 10.1300/J175v02n02_04, Full text, Accessed on: 8 November 2014.</ref> and in humans, dried leaves of cannabis were used to treat nose bleeds, and cannabis seeds were used to expel tapeworms.<ref name="hawthorne" />
In the medieval Islamic world, Arabic physicians made use of the diuretic, antiemetic, antiepileptic, anti-inflammatory, analgesic and antipyretic properties of Cannabis sativa, and used it extensively as medication from the 8th to 18th centuries.<ref>,
The Therapeutic Use of Cannabis sativa (L.) in Arabic Medicine, Journal of Cannabis Therapeutics, 2001, Vol. 1, pp. 63–70, DOI: 10.1300/J175v01n01_05,</ref>
Landrace strains

Cannabis seeds may have been used for food, rituals or religious practices in ancient Europe and China.<ref name = "Holland_2018">,
The Pot Book: A Complete Guide to Cannabis. online version, New York:Simon and Schuster, ISBN 978-1-59477-898-8, Accessed: 22 April 2018.</ref>: 19–22 Harvesting the plant led to the spread of cannabis throughout Eurasia about 10,000 to 5,000 years ago, with further distribution to the Middle East and Africa about 2,000 to 500 years ago.<ref name = "Holland_2018" />: 18–19 A landrace strain of cannabis developed over centuries.<ref>, Raven Biology of Plants, 8th edition, New York:W. H. Freeman and Company, ISBN 978-1-4292-1961-7, Pages: 213–17,</ref> They are cultivars of the plant that originated in one specific region.
Widely cultivated strains of cannabis, such as "Afghani" or "Hindu Kush", are indigenous to the Pakistan and Afghanistan regions, while "Durban Poison" is native to Africa.<ref name = "Holland_2018" />: 45–48 There are approximately 16 landrace strains of cannabis identified from Pakistan, Jamaica, Africa, Mexico, Central America and Asia.<ref>,
Raven Biology of Plants, 8th edition, New York:W.H. Freeman and Company, ISBN 978-1-4292-1961-7, Pages: 501–04,</ref>
Modern
An Irish physician, William Brooke O'Shaughnessy, is credited with introducing cannabis to Western medicine.<ref name=Mack>,
Marijuana As Medicine?: The Science Beyond the Controversy. online version, National Academies Press, 2000, ISBN 978-0-309-06531-3, Accessed: 20 December 2015. Pages: 15–,</ref> O'Shaughnessy discovered cannabis in the 1830s while living abroad in India, where he conducted numerous experiments investigating the drug's medical utility (noting in particular its analgesic and anticonvulsant effects).<ref name="Booth">, Cannabis: A History, New York:St. Martin's Press, 2005, ISBN 978-0-312-42494-7,</ref> He returned to England with a supply of cannabis in 1842, after which its use spread through Europe and the United States.<ref name="Grinspoon">, Marihuana, the Forbidden Medicine, Revised and expanded edition, Yale University Press, ISBN 978-0-300-07086-6,</ref> In 1845 French physician Jacques-Joseph Moreau published a book about the use of cannabis in psychiatry.<ref>Hans Bangen:Geschichte der medikamentösen Therapie der Schizophrenie. Berlin 1992, p. 22.</ref> In 1850 cannabis was entered into the United States Pharmacopeia.<ref name="Booth" /> An anecdotal report of Cannabis indica as a treatment for tetanus appeared in Scientific American in 1880.<ref>, Scientific American, "Successful Treatment of Tetanus". online version, Munn & Company, Accessed: 5 June 2021.</ref>
The use of cannabis in medicine began to decline by the end of the 19th century, due to difficulty in controlling dosages and the rise in popularity of synthetic and opium-derived drugs.<ref name="Grinspoon" /> Also, the advent of the hypodermic syringe allowed these drugs to be injected for immediate effect, in contrast to cannabis which is not water-soluble and therefore cannot be injected.<ref name="Grinspoon" />
In the United States, the medical use of cannabis further declined with the passage of the Marihuana Tax Act of 1937, which imposed new regulations and fees on physicians prescribing cannabis.<ref>,
State Medical Marijuana Laws: Understanding the Laws and Their Limitations, Journal of Public Health Policy, Vol. 23(Issue: 4), pp. 413–39, DOI: 10.2307/3343240, PMID: 12532682, Full text, Accessed on: 20 March 2018.</ref> Cannabis was removed from the U.S. Pharmacopeia in 1941, and officially banned for any use with the passage of the Controlled Substances Act of 1970.<ref name="Grinspoon" />
Cannabis began to attract renewed interest as medicine in the 1970s and 1980s, in particular due to its use by cancer and AIDS patients who reported relief from the effects of chemotherapy and wasting syndrome.<ref> ,
Marijuana and Medicine – Assessing the Science Base Full text, , National Academy Press, 1999, Washington, D.C., Accessed on: 28 July 2017.
</ref> In 1996, California became the first U.S. state to legalize medical cannabis in defiance of federal law.<ref>
History of Marijuana as Medicine – 2900 BC to Present(link). ProCon.org.
Accessed 27 July 2017.
</ref> In 2001, Canada became the first country to adopt a system regulating the medical use of cannabis.<ref>
,
Marijuana's journey to legal health treatment: the Canadian experience Full text, CBC News, 17 August 2009, Accessed on: 27 July 2017.
</ref>
-

-
 Cannabis indica fluid extract, American Druggists Syndicate, pre-1937
Cannabis indica fluid extract, American Druggists Syndicate, pre-1937 -
 An advertisement for cannabis americana distributed by a pharmacist in New York in 1917
An advertisement for cannabis americana distributed by a pharmacist in New York in 1917 -
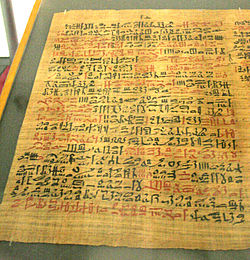 The Ebers Papyrus (c. 1550 BCE) from Ancient Egypt has a prescription for medical marijuana applied directly for inflammation.
The Ebers Papyrus (c. 1550 BCE) from Ancient Egypt has a prescription for medical marijuana applied directly for inflammation.




Society and culture
Legal status

See also countries that have decriminalized or where enforcement is limited.
Countries that have legalized the medical use of cannabis include Argentina,<ref> ,
Argentina to Allow Medicinal Marijuana to Be Grown at Home Full text, The New York Times, 12 November 2020, Accessed on: 22 January 2023.
</ref> Australia,<ref> ,
Medicinal Marijuana Legal In Australia Full text, Canstar, 28 February 2018, Accessed on: 16 July 2018.
</ref> Brazil,<ref> ,
Brazil Regulates Sale Of Medical Marijuana Products Full text, Benzinga, 3 December 2019, Accessed on: 10 December 2019.
</ref> Canada,<ref name="Motley"> ,
10 Countries (Aside From the U.S.) Where Some Form of Medical Marijuana Is Legal Full text, The Motley Fool, 15 May 2016, Accessed on: 5 November 2017.
</ref> Chile,<ref name="Motley" /> Colombia,<ref name="Motley" /> Costa Rica,<ref> ,
Costa Rica legalizes medicinal marijuana use, hemp growing Full text, Associated Press, 2 March 2022, Accessed on: 22 January 2023.
</ref> Croatia,<ref> ,
Croatia legalises marijuana for medical use Full text, Yahoo News, 15 October 2015, Accessed on: 4 November 2017.
</ref> Cyprus,<ref> ,
Cyprus begins to distribute medical cannabis Full text, InCyprus, 22 May 2017, Accessed on: 11 November 2017.
</ref> Czech Republic,<ref name="Motley" /> Finland,<ref>
Legal status of cannabis in Finland – An overview(link). Sensi Seeds.
Accessed 4 November 2017.
</ref> Germany,<ref>
,
Germany joins the global experiment on marijuana legalization Full text, CNN.com, 6 March 2017, Accessed on: 4 November 2017.
</ref> Greece,<ref> ,
Greece legalises marijuana for medical purposes Full text, The Independent, 3 July 2017, Accessed on: 4 November 2017.
</ref> Israel,<ref> ,
How the Booming Israeli Weed Industry Is Changing American Pot Full text, Rollingstone.com, 24 August 2017, Accessed on: 4 November 2017.
</ref> Italy,<ref> Samuels, Gabriel,
Italian army aims to produce "the best-quality" medical marijuana after finding current batches deficient Full text, The Independent, 26 July 2016, Accessed on: 4 November 2017.
</ref> Jamaica,<ref> ,
Jamaica's Kaya Farms Becomes First Medical Marijuana Dispensary To Open Full text, marijuana.com, 19 March 2018, Accessed on: 16 July 2018.
</ref> Lebanon,<ref> ,
Lebanon Legalizes Cannabis Farming for Medicinal Use Full text, The New York Times, 21 April 2020, Accessed on: 25 April 2020.
</ref> Luxembourg,<ref> ,
Cannabis for medical use legalised in Luxembourg Full text, Luxembourg Times, 29 June 2018, Accessed on: 8 July 2018.
</ref> Malta,<ref> ,
Malta has officially legalised medical cannabis Full text, Malta Today, 27 March 2018, Accessed on: 24 August 2018.
</ref> Morocco,<ref> ,
Morocco: Bill to legalise cannabis enters into force Full text, Middle East Monitor, 31 July 2021, Accessed on: 22 January 2023.
</ref> the Netherlands,<ref name="Motley" /> New Zealand,<ref> ,
New Zealand passes laws to make medical marijuana widely available Full text, The Guardian, 11 December 2018, Accessed on: 20 January 2019.
</ref> North Macedonia,<ref> ,
Macedonia Allows Medical Marijuana in Pharmacies Full text, Balkan Insight, 1 June 2016, Accessed on: 4 November 2017.
</ref> Panama,<ref> ,
El gobierno de Panamá legalizó el uso medicinal y terapéutico del cannabis Full text, Infobae, 14 October 2021, Accessed on: 22 January 2023.
</ref> Peru,<ref> ,
Peru legalises medical marijuana in move spurred by mother's home lab Full text, The Guardian, 20 October 2017, Accessed on: 4 Nov 2017.
</ref> Poland,<ref> ,
Medical use of cannabis officially legal in Poland Full text, Radio Poland, 11 February 2017, Accessed on: 4 November 2017.
</ref> Portugal,<ref> ,
Portugal passes medical cannabis law, opens domestic market Full text, Marijuana Business Daily, 21 June 2018, Accessed on: 24 August 2018.
</ref> Rwanda,<ref> ,
10 things to know after Rwanda gives the green light for medical marijuana Full text, The New Times, 29 June 2021, Accessed on: 22 January 2023.
</ref> Sri Lanka,<ref> </ref> Switzerland,<ref> ,
Switzerland to legalise medicinal cannabis from Monday Full text, The Local, 28 July 2022, Accessed on: 22 January 2023.
</ref> Thailand,<ref> ,
Thailand Approves Medical Marijuana In Regional First Full text, HuffPost, 25 December 2018, Accessed on: 20 January 2019.
</ref> the United Kingdom,<ref> ,
Medicinal cannabis products to be legalised Full text, BBC, 26 July 2018, Accessed on: 28 July 2018.
</ref> and Uruguay.<ref name="Motley" /> Other countries have more restrictive laws that allow only the use of isolated cannabinoid drugs such as Sativex or Epidiolex.<ref>
Sativex (delta-9-tetrahydrocannabinol and cannabidiol)(link). GW Pharmaceuticals.
Accessed 5 November 2017.
</ref><ref>
</ref> Countries with the most relaxed policies include Canada,<ref>
Sapra, Bani,
Canada becomes second nation in the world to legalize marijuana Full text, CNN, 20 June 2018, Accessed on: 3 July 2018.
</ref> the Netherlands,<ref name="Motley" /> Thailand,<ref> ,
Weed Is Now Legal in Thailand. How Long Will the High Times Last? Full text, The New York Times, 10 November 2022, Accessed on: 22 January 2023.
</ref> and Uruguay,<ref name="Motley" /> where cannabis can be purchased without need for a prescription. In Mexico, THC content of medical cannabis is limited to one percent.<ref> ,
Legal Pot In Mexico: Everything You Need to Know Full text, , 14 September 2017, Accessed on: 5 November 2017.
</ref> In the United States, the legality of medical cannabis varies by state.<ref name="NCSL" />
However, in many of these countries, access may not always be possible under the same conditions.
International law
Cannabis and its derivatives are subject to regulation under three United Nations drug control treaties: the 1961 Single Convention on Narcotic Drugs, the 1971 Convention on Psychotropic Substances, and the 1988 Convention Against Illicit Traffic in Narcotic Drugs and Psychotropic Substances.<ref>,
Legalizing Cannabis Violates the UN Drug Control Treaties, But Progressive Countries Like Canada Have Options, Ottawa Law Review, Vol. 49(Issue: 2), Full text, Accessed on: 8 January 2021.</ref>
Cannabis and cannabis resin are classified as a Schedule I drug under the Single Convention treaty, meaning that medical use is considered "indispensible for the relief of pain and suffering" but that it is considered to be an addictive medication with risks of abuse.<ref>
Classification of controlled drugs(link). European Monitoring Centre for Drugs and Drug Addiction.
Accessed 7 January 2021.
</ref> Countries have an obligation to provide access and sufficient availability of drugs listed in Schedule I for the purposes of medical uses.<ref>,
Report of the International Narcotics Control Board on the Availability of Internationally Controlled Drugs: Ensuring Adequate Access for Medical and Scientific Purposes. online version, Vienna:United Nations, 2010,</ref><ref>
International Centre on Human Rights and Drug Policy (University of Essex), United Nations Development Programme, Joint United Nations Programme on HIV/AIDS, Office of the United Nations High Commissioner for Human Rights, World Health Organization. Obligations arising from human rights standards: Access to controlled substances as medicines(link). International Guidelines on Human Rights and Drug Policy.
2012.
Accessed 2024-08-30.
</ref>
Prior to December 2020 cannabis and cannabis resin were also included in Schedule IV, a more restrictive level of control, which is for only the most dangerous drugs such as heroin and fentanyl.<ref> ,
The UN removes cannabis from a list of the most dangerous substances Full text, CNN, 2 December 2020, Accessed on: 7 January 2021.
</ref> They were removed after an independent scientific assessment by the World Health Organization in 2018-1029.
Member nations of the UN Commission on Narcotic Drugs voted 27–25 to remove it from Schedule IV on 2 December 2020,<ref> ,
U.N. Reclassifies Cannabis as a Less Dangerous Drug Full text, The New York Times, 2 December 2020, Accessed on: 7 January 2021.
</ref> following a World Health Organization recommendation for removal in January 2019.<ref> ,
WHO recommends rescheduling of cannabis Full text, European Monitoring Centre for Drugs and Drug Addiction, 25 March 2019, Accessed on: 7 January 2021.
</ref><ref> ,
WHO Recommends Rescheduling Cannabis in International Law for First Time in History Full text, Newsweek, 8 February 2019, Accessed on: 7 January 2021.
</ref>
United States
In the United States, the use of cannabis for medical purposes is legal in 38 states, four out of five permanently inhabited U.S. territories, and the District of Columbia.<ref name="NCSL">
State Medical Marijuana Laws(link). National Conference of State Legislatures.
12 September 2022.
Accessed 6 October 2022.
</ref> An additional 10 states have more restrictive laws allowing the use of low-THC products.<ref name="NCSL" /> Cannabis remains illegal at the federal level under the Controlled Substances Act, which classifies it as a Schedule I drug with a high potential for abuse and no accepted medical use. In December 2014, however, the Rohrabacher–Farr amendment was signed into law, prohibiting the Justice Department from prosecuting individuals acting in accordance with state medical cannabis laws.<ref>
,
Jeff Sessions personally asked Congress to let him prosecute medical-marijuana providers Full text, , 13 June 2017, Accessed on: 9 July 2017.
</ref>
In the US, the FDA has approved two oral cannabinoids for use as medicine in 1985:<ref> ,
"New" Pot Pill For Chemo Patients Full text, CBS News, 16 May 2006, Accessed on: 26 July 2017.
</ref> dronabinol (pure delta-9-THC; brand name Marinol) and nabilone (a synthetic neocannabinoid; brand name Cesamet).<ref name="Borgelt2013" /> In the US, they are both listed as Schedule II, indicating high potential for side effects and addiction.<ref name="Svrakic2012" /><ref>
Final Rule: Placement of FDA-Approved Products of Oral Solutions Containing Dronabinol [(-)-delta-9-trans-tetrahydrocannabinol (delta-9-THC)] in Schedule II(link). U.S. Department of Justice.
Accessed 2 February 2018.
</ref>
Economics
Distribution

The method of obtaining medical cannabis varies by region and by legislation. In the US, most consumers grow their own or buy it from cannabis dispensaries in states where it is legal.<ref name=Borgelt2013 /><ref name=BaltSun> Timothy B. Wheeler,
Medical marijuana fees stir debate in Maryland Full text, , 11 October 2014, Accessed on: 12 October 2014.
</ref> Marijuana vending machines for selling or dispensing cannabis are in use in the United States and are planned to be used in Canada.<ref name=FirstForeignMarket> Blackwell, Tom,
The pot vending machine's first foreign market? Canada, of course, "a seed for the rest of the world" Full text, , 16 October 2013, Accessed on: 4 December 2013.
</ref> In 2014, the startup Meadow began offering on-demand delivery of medical marijuana in the San Francisco Bay Area, through their mobile app.<ref>
Uber-For-Weed Startup Meadow Lights Up In San Francisco(link). {{{website}}}. AOL. 14 October 2014.
Accessed 22 January 2016.
</ref>
Almost 70% of medical cannabis is exported from the United Kingdom, according to a 2017 United Nations report, with much of the remaining amount coming from Canada and the Netherlands.<ref>
The UK is the world's largest producer of legal Cannabis, UN body finds(link). The Independent.
2018-03-07.
Accessed 2020-12-07.
</ref>
Insurance
In the United States, health insurance companies may not pay for a medical marijuana prescription as the Food and Drug Administration must approve any substance for medicinal purposes. Before this can happen, the FDA must first permit the study of the medical benefits and drawbacks of the substance, which it has not done since it was placed on Schedule I of the Controlled Substances Act in 1970. Therefore, all expenses incurred fulfilling a medical marijuana prescription will possibly be incurred as out-of-pocket.<ref>
The Medical Marijuana Debate(link). Compliance Corner. Wolters Kluwer Financial Services. 10 February 2015.
Accessed 26 February 2015.
</ref> However, the New Mexico Court of Appeals has ruled that workers' compensation insurance must pay for prescribed marijuana as part of the state's Medical Cannabis Program.<ref>
Court: Employer can't block workers' comp for medical marijuana(link). NM Political Report.
29 June 2015.
Accessed 30 June 2015.
</ref>
Positions of medical organizations
Medical organizations that have issued statements in support of allowing access to medical cannabis include the American Nurses Association,<ref name="ANA"> </ref> American Public Health Association,<ref>
Resolution on Medical Marijuana(link). druglibrary.org.
Accessed 30 July 2017.
</ref> American Medical Student Association,<ref>
House of Delegates 2017, Resolution: A8(link). amsa.org. American Medical Student Association.
Accessed 30 July 2017.
</ref> National Multiple Sclerosis Society,<ref>
Medical Marijuana (Cannabis) FAQs(link). National Multiple Sclerosis Society.
Accessed 30 July 2017.
</ref> Epilepsy Foundation,<ref>
</ref> and Leukemia & Lymphoma Society.<ref>
Medical Marijuana Use and Research(link). maps.org. Leukemia & Lymphoma Society.
Accessed 30 July 2017.
</ref>
Organizations that oppose the legalization of medical cannabis include the American Academy of Pediatrics (AAP)<ref name="AAP"> </ref> and American Psychiatric Association.<ref>
Position Statement on Marijuana as Medicine(link). American Psychiatric Association.
Accessed 30 July 2017.
</ref> However, the AAP also supports rescheduling for the purpose of facilitating research.<ref name="AAP" />
The American Medical Association<ref> </ref> and American College of Physicians<ref> </ref> do not take a position on the legalization of medical cannabis, but have called for the Schedule I classification to be reviewed. The American Academy of Family Physicians<ref name="AAFP"> ,
AAFP Releases Marijuana, Cannabinoids Position Paper Full text, American Academy of Family Physicians, 20 September 2019, Accessed on: 6 October 2019.
</ref> and American Society of Addiction Medicine<ref> </ref> also do not take a position, but do support rescheduling to better facilitate research. The American Heart Association says that "many of the concerning health implications of cannabis include cardiovascular diseases" but that it supports rescheduling to allow "more nuanced ... marijuana legislation and regulation" and to "reflect the existing science behind cannabis".<ref>American Heart Association,
Medical Marijuana, Recreational Cannabis, and Cardiovascular Health, Circulation, Vol. 142(Issue: 10), pp. e131–52, DOI: 10.1161/CIR.0000000000000883, PMID: 32752884,</ref> The American Cancer Society<ref name="ACS">
Marijuana and Cancer(link). American Cancer Society.
Accessed 12 July 2017.
</ref> and American Psychological Association<ref name="APA">
,
Marijuana research: Overcoming the barriers Full text, American Psychological Association, 14 September 2017, Accessed on: 9 October 2017.
</ref> have noted the obstacles that exist for conducting research on cannabis, and have called on the federal government to better enable scientific study of the drug.
Cancer Research UK say that while cannabis is being studied for therapeutic potential, "claims that there is solid "proof" that cannabis or cannabinoids can cure cancer is highly misleading to patients and their families, and builds a false picture of the state of progress in this area".<ref> Arney, Kat. Cannabis, cannabinoids and cancer – the evidence so far(link). {{{website}}}. Cancer Research UK. 25 July 2012.
</ref>
Nonproprietary names
There are three International Nonproprietary Name (INN) granted for cannabinoids: two plant-derived phytocannabinoids and one neocannabinoid:
- Dronabinol is the INN for delta-9-THC<ref>World Health Organization,
List of Proposed INNs No. 51, WHO Chronicle, Vol. 38(Issue: 2), Full text,</ref><ref>World Health Organization, List of Recommended INNs No. 24, WHO Chronicle, Vol. 38(Issue: 6), Full text,</ref> (there is a common confusion according to which the word "dronabinol" would only refer to synthetic delta-9-THC, which is incorrect<ref>Riboulet-Zemouli, Kenzi, 'Cannabis' ontologies I: Conceptual issues with Cannabis and cannabinoids terminology, Drug Science, Policy and Law, Vol. 6, pp. 205032452094579, DOI: 10.1177/2050324520945797, Full text,</ref>).
- Cannabidiol is also the official INN for the molecule, granted in 2017.<ref>World Health Organization,
List of Recommended INNs No. 77, WHO Drug Information, Vol. 31(Issue: 1), Full text,</ref>
Nabiximols is the generic name (but not recognized as an INN) of a mixture of Cannabidiol and Dronabinol. Its most common form is the oromucosal spray derived from two strains of Cannabis sativa and containing THC and CBD traded under the brand name Sativex®.<ref name="Svrakic2012" /> It is not approved in the United States, but is approved in several European countries, Canada, and New Zealand as of 2013.<ref name="Borgelt2013" />
| Generic name |
Brand name(s) |
Country (non-exhaustive) | Licensed indications |
|---|---|---|---|
| Nabilone | Cesamet | U.S., Canada | Antiemetic (treatment of nausea or vomiting) associated with chemotherapy that has failed to respond adequately to conventional therapy<ref name=Borgelt2013 /> |
| Dronabinol | Marinol | ||
| Syndros | U.S. | Anorexia associated with AIDS–related weight loss<ref name=Borgelt2013 /> | |
| Nabiximols | Sativex | Canada, New Zealand, majority of the EU<ref>, Medical use of cannabis and cannabinoids containing products – Regulations in Europe and North America, European Journal of Internal Medicine, Vol. 49, pp. 2–6, DOI: 10.1016/j.ejim.2018.01.001, PMID: 29329891,</ref> |
Limited treatment for spasticity and neuropathic pain associated with multiple sclerosis and intractable cancer pain.<ref name=Borgelt2013 /> |
As an antiemetic, these medications are usually used when conventional treatment for nausea and vomiting associated with cancer chemotherapy fail to work.<ref name=Borgelt2013 />
Nabiximols is used for treatment of spasticity associated with MS when other therapies have not worked, and when an initial trial demonstrates "meaningful improvement".<ref name=Borgelt2013 /> Trials for FDA approval in the US are underway.<ref name=Borgelt2013 /> It is also approved in several European countries for overactive bladder and vomiting.<ref name=Svrakic2012 /> When sold under the trade name Sativex as a mouth spray, the prescribed daily dose in Sweden delivers a maximum of 32.4 mg of THC and 30 mg of CBD; mild to moderate dizziness is common during the first few weeks.<ref>
Produkt – FASS Allmänhet(link). {{{website}}}.
Accessed 26 December 2013.
</ref>
Relative to inhaled consumption, peak concentration of oral THC is delayed, and it may be difficult to determine optimal dosage because of variability in patient absorption.<ref name=Borgelt2013 />
In 1964, Albert Lockhart and Manley West began studying the health effects of traditional cannabis use in Jamaican communities. They developed, and in 1987 gained permission to market, the pharmaceutical "Canasol", one of the first cannabis extracts.<ref name="FFY"> Youssef, Farid F.. Cannabis Unmasked: What it is and why it does what it does(link). {{{website}}}.
June 2010.
Accessed 11 May 2021.
</ref>
Research
A 2022 review concluded that "oral, synthetic cannabis products with high THC-to-CBD ratios and sublingual, extracted cannabis products with comparable THC-to-CBD ratios may be associated with short-term improvements in chronic pain and increased risk for dizziness and sedation."<ref name="pmid35667066">,
Cannabis-Based Products for Chronic Pain: A Systematic Review, Ann Intern Med, 2022, Vol. 175(Issue: 8), pp. 1143–1153, DOI: 10.7326/M21-4520, PMID: 35667066, Full text, Accessed on: 19 February 2023.</ref>
See also
Lua error: bad argument #2 to 'title.new' (unrecognized namespace name 'Portal').
References
Further reading
- ,
The Health Effects of Cannabis and Cannabinoids: The Current State of Evidence and Recommendations for Research. online version, National Academies of Sciences, Engineering, and Medicine: The National Academies Press, ISBN 978-0-309-45304-2, DOI: 10.17226/24625, Accessed: 7 February 2017.
External links
, links to websites about medical cannabis
- Information on Cannabis and Cannabinoids from the U.S. National Cancer Institute
- Information on cannabis (marihuana, marijuana) and the cannabinoids from Health Canada
- The Center for Medicinal Cannabis Research of the University of California
- Medical Marijuana – a 2014–2015 three-part CNN documentary produced by Sanjay Gupta
- Template:NYTtopic
| Cannabis | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
*
|
Ad. Transform your life with W8MD's
GLP-1 weight loss injections special from $29.99 with insurance
|
WikiMD Medical Encyclopedia |
Medical Disclaimer: WikiMD is for informational purposes only and is not a substitute for professional medical advice. Content may be inaccurate or outdated and should not be used for diagnosis or treatment. Always consult your healthcare provider for medical decisions. Verify information with trusted sources such as CDC.gov and NIH.gov. By using this site, you agree that WikiMD is not liable for any outcomes related to its content. See full disclaimer.
Credits:Most images are courtesy of Wikimedia commons, and templates, categories Wikipedia, licensed under CC BY SA or similar.
Translate this page: - East Asian
中文,
日本,
한국어,
South Asian
हिन्दी,
தமிழ்,
తెలుగు,
Urdu,
ಕನ್ನಡ,
Southeast Asian
Indonesian,
Vietnamese,
Thai,
မြန်မာဘာသာ,
বাংলা
European
español,
Deutsch,
français,
Greek,
português do Brasil,
polski,
română,
русский,
Nederlands,
norsk,
svenska,
suomi,
Italian
Middle Eastern & African
عربى,
Turkish,
Persian,
Hebrew,
Afrikaans,
isiZulu,
Kiswahili,
Other
Bulgarian,
Hungarian,
Czech,
Swedish,
മലയാളം,
मराठी,
ਪੰਜਾਬੀ,
ગુજરાતી,
Portuguese,
Ukrainian
- Pages with script errors
- Wikipedia pages with incorrect protection templates
- Use American English from October 2017
- Articles with invalid date parameter in template
- All Wikipedia articles written in American English
- Articles with specifically marked weasel-worded phrases from April 2017
- Articles with hatnote templates targeting a nonexistent page
- Articles containing potentially dated statements from 2021
- All articles containing potentially dated statements
- Articles containing potentially dated statements from 2013
- Wikipedia articles needing page number citations from August 2010
- Medicinal use of cannabis
- Antiemetics
- Antioxidants
- Biologically based therapies
- Herbalism
- Medical ethics
- Medicinal plants
- Pharmaceuticals policy
- Pharmacognosy

{kind=link}