Permanent junctional reciprocating tachycardia: Difference between revisions
CSV import |
CSV import |
||
| Line 1: | Line 1: | ||
{{SI}} | |||
{{Infobox medical condition | |||
| name = Permanent junctional reciprocating tachycardia | |||
| image = [[File:AVRT.tif|left|thumb|Illustration of atrioventricular reentrant tachycardia]] | |||
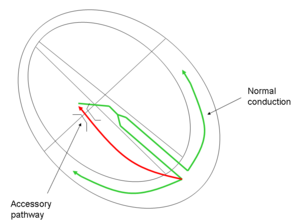
| caption = Illustration of atrioventricular reentrant tachycardia | |||
| field = [[Cardiology]] | |||
| synonyms = PJRT | |||
| symptoms = [[Palpitations]], [[dizziness]], [[syncope]], [[shortness of breath]] | |||
| complications = [[Heart failure]], [[cardiomyopathy]] | |||
| onset = Childhood or adolescence | |||
| duration = Chronic | |||
| causes = [[Accessory pathway]] | |||
| risks = [[Congenital heart disease]], [[genetic predisposition]] | |||
| diagnosis = [[Electrocardiogram]], [[Holter monitor]], [[electrophysiological study]] | |||
| differential = [[Atrioventricular nodal reentrant tachycardia]], [[atrial fibrillation]], [[ventricular tachycardia]] | |||
| prevention = None | |||
| treatment = [[Medications]], [[catheter ablation]], [[surgery]] | |||
| medication = [[Beta blockers]], [[calcium channel blockers]], [[antiarrhythmic drugs]] | |||
| prognosis = Good with treatment | |||
| frequency = Rare | |||
}} | |||
{{Short description|A type of supraventricular tachycardia}} | {{Short description|A type of supraventricular tachycardia}} | ||
'''Permanent junctional reciprocating tachycardia''' (PJRT) is a rare form of [[supraventricular tachycardia]] (SVT) characterized by a reentrant circuit involving an [[accessory pathway]] that conducts in a retrograde manner. This condition is typically seen in children but can persist into adulthood. Unlike other forms of SVT, PJRT is often incessant, meaning it occurs continuously or very frequently, which can lead to [[tachycardia-induced cardiomyopathy]]. | '''Permanent junctional reciprocating tachycardia''' (PJRT) is a rare form of [[supraventricular tachycardia]] (SVT) characterized by a reentrant circuit involving an [[accessory pathway]] that conducts in a retrograde manner. This condition is typically seen in children but can persist into adulthood. Unlike other forms of SVT, PJRT is often incessant, meaning it occurs continuously or very frequently, which can lead to [[tachycardia-induced cardiomyopathy]]. | ||
==Pathophysiology== | ==Pathophysiology== | ||
PJRT is caused by the presence of an [[accessory pathway]] that connects the [[atrium]] and [[ventricle]] outside of the normal [[atrioventricular node]] conduction system. This accessory pathway conducts electrical impulses from the ventricles back to the atria, creating a reentrant circuit. The pathway in PJRT is typically located in the posteroseptal region of the heart and has decremental conduction properties, meaning its conduction speed decreases with increasing heart rates. | PJRT is caused by the presence of an [[accessory pathway]] that connects the [[atrium]] and [[ventricle]] outside of the normal [[atrioventricular node]] conduction system. This accessory pathway conducts electrical impulses from the ventricles back to the atria, creating a reentrant circuit. The pathway in PJRT is typically located in the posteroseptal region of the heart and has decremental conduction properties, meaning its conduction speed decreases with increasing heart rates. | ||
==Clinical Presentation== | ==Clinical Presentation== | ||
Patients with PJRT often present with symptoms of [[palpitations]], [[fatigue]], and [[dyspnea]]. In infants and young children, it may present as [[congestive heart failure]] due to the persistent tachycardia. Older children and adults may experience exercise intolerance and palpitations. The incessant nature of the tachycardia can lead to [[tachycardia-induced cardiomyopathy]], which can cause [[heart failure]] if not treated. | Patients with PJRT often present with symptoms of [[palpitations]], [[fatigue]], and [[dyspnea]]. In infants and young children, it may present as [[congestive heart failure]] due to the persistent tachycardia. Older children and adults may experience exercise intolerance and palpitations. The incessant nature of the tachycardia can lead to [[tachycardia-induced cardiomyopathy]], which can cause [[heart failure]] if not treated. | ||
==Diagnosis== | ==Diagnosis== | ||
The diagnosis of PJRT is typically made using [[electrocardiography]] (ECG). The ECG in PJRT shows a narrow complex tachycardia with a long RP interval, which is the time between the onset of the P wave and the preceding R wave. This is due to the retrograde conduction through the accessory pathway. [[Electrophysiological study]] can be used to confirm the diagnosis and to locate the accessory pathway. | The diagnosis of PJRT is typically made using [[electrocardiography]] (ECG). The ECG in PJRT shows a narrow complex tachycardia with a long RP interval, which is the time between the onset of the P wave and the preceding R wave. This is due to the retrograde conduction through the accessory pathway. [[Electrophysiological study]] can be used to confirm the diagnosis and to locate the accessory pathway. | ||
==Management== | ==Management== | ||
The management of PJRT involves controlling the heart rate and, if possible, eliminating the accessory pathway. [[Beta blockers]] and [[calcium channel blockers]] are often used to control the heart rate. [[Antiarrhythmic drugs]] such as [[flecainide]] or [[amiodarone]] may be used in some cases. The definitive treatment for PJRT is [[radiofrequency catheter ablation]] of the accessory pathway, which can cure the condition by interrupting the reentrant circuit. | The management of PJRT involves controlling the heart rate and, if possible, eliminating the accessory pathway. [[Beta blockers]] and [[calcium channel blockers]] are often used to control the heart rate. [[Antiarrhythmic drugs]] such as [[flecainide]] or [[amiodarone]] may be used in some cases. The definitive treatment for PJRT is [[radiofrequency catheter ablation]] of the accessory pathway, which can cure the condition by interrupting the reentrant circuit. | ||
==Prognosis== | ==Prognosis== | ||
With appropriate treatment, the prognosis for patients with PJRT is generally good. Radiofrequency ablation has a high success rate and can prevent the recurrence of tachycardia. If left untreated, PJRT can lead to [[heart failure]] and other complications due to the persistent tachycardia. | With appropriate treatment, the prognosis for patients with PJRT is generally good. Radiofrequency ablation has a high success rate and can prevent the recurrence of tachycardia. If left untreated, PJRT can lead to [[heart failure]] and other complications due to the persistent tachycardia. | ||
==See also== | |||
== | |||
* [[Supraventricular tachycardia]] | * [[Supraventricular tachycardia]] | ||
* [[Atrioventricular reentrant tachycardia]] | * [[Atrioventricular reentrant tachycardia]] | ||
* [[Accessory pathway]] | * [[Accessory pathway]] | ||
* [[Electrophysiological study]] | * [[Electrophysiological study]] | ||
[[Category:Cardiac arrhythmia]] | [[Category:Cardiac arrhythmia]] | ||
[[Category:Supraventricular tachycardia]] | [[Category:Supraventricular tachycardia]] | ||
Latest revision as of 15:30, 8 April 2025

Editor-In-Chief: Prab R Tumpati, MD
Obesity, Sleep & Internal medicine
Founder, WikiMD Wellnesspedia &
W8MD medical weight loss NYC and sleep center NYC
| Permanent junctional reciprocating tachycardia | |
|---|---|
 | |
| Synonyms | PJRT |
| Pronounce | N/A |
| Specialty | N/A |
| Symptoms | Palpitations, dizziness, syncope, shortness of breath |
| Complications | Heart failure, cardiomyopathy |
| Onset | Childhood or adolescence |
| Duration | Chronic |
| Types | N/A |
| Causes | Accessory pathway |
| Risks | Congenital heart disease, genetic predisposition |
| Diagnosis | Electrocardiogram, Holter monitor, electrophysiological study |
| Differential diagnosis | Atrioventricular nodal reentrant tachycardia, atrial fibrillation, ventricular tachycardia |
| Prevention | None |
| Treatment | Medications, catheter ablation, surgery |
| Medication | Beta blockers, calcium channel blockers, antiarrhythmic drugs |
| Prognosis | Good with treatment |
| Frequency | Rare |
| Deaths | N/A |
A type of supraventricular tachycardia
Permanent junctional reciprocating tachycardia (PJRT) is a rare form of supraventricular tachycardia (SVT) characterized by a reentrant circuit involving an accessory pathway that conducts in a retrograde manner. This condition is typically seen in children but can persist into adulthood. Unlike other forms of SVT, PJRT is often incessant, meaning it occurs continuously or very frequently, which can lead to tachycardia-induced cardiomyopathy.
Pathophysiology[edit]
PJRT is caused by the presence of an accessory pathway that connects the atrium and ventricle outside of the normal atrioventricular node conduction system. This accessory pathway conducts electrical impulses from the ventricles back to the atria, creating a reentrant circuit. The pathway in PJRT is typically located in the posteroseptal region of the heart and has decremental conduction properties, meaning its conduction speed decreases with increasing heart rates.
Clinical Presentation[edit]
Patients with PJRT often present with symptoms of palpitations, fatigue, and dyspnea. In infants and young children, it may present as congestive heart failure due to the persistent tachycardia. Older children and adults may experience exercise intolerance and palpitations. The incessant nature of the tachycardia can lead to tachycardia-induced cardiomyopathy, which can cause heart failure if not treated.
Diagnosis[edit]
The diagnosis of PJRT is typically made using electrocardiography (ECG). The ECG in PJRT shows a narrow complex tachycardia with a long RP interval, which is the time between the onset of the P wave and the preceding R wave. This is due to the retrograde conduction through the accessory pathway. Electrophysiological study can be used to confirm the diagnosis and to locate the accessory pathway.
Management[edit]
The management of PJRT involves controlling the heart rate and, if possible, eliminating the accessory pathway. Beta blockers and calcium channel blockers are often used to control the heart rate. Antiarrhythmic drugs such as flecainide or amiodarone may be used in some cases. The definitive treatment for PJRT is radiofrequency catheter ablation of the accessory pathway, which can cure the condition by interrupting the reentrant circuit.
Prognosis[edit]
With appropriate treatment, the prognosis for patients with PJRT is generally good. Radiofrequency ablation has a high success rate and can prevent the recurrence of tachycardia. If left untreated, PJRT can lead to heart failure and other complications due to the persistent tachycardia.
