Sessile serrated lesion: Difference between revisions
CSV import Tags: mobile edit mobile web edit |
CSV import |
||
| Line 27: | Line 27: | ||
{{Medicine-stub}} | {{Medicine-stub}} | ||
<gallery> | |||
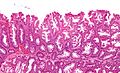
File:Sessile serrated adenoma 3 very high mag.jpg|Sessile serrated lesion | |||
File:Sessile serrated adenoma 3 low mag.jpg|Sessile serrated lesion | |||
File:Sessile serrated adenoma 3 intermed mag.jpg|Sessile serrated lesion | |||
File:Sessile serrated adenoma 2 high mag.jpg|Sessile serrated lesion | |||
</gallery> | |||
Revision as of 01:15, 20 February 2025
Sessile Serrated Lesion (SSL) is a type of colorectal polyp that is considered a precursor to colorectal cancer, specifically through the serrated pathway. SSLs are characterized by their sessile (flat) appearance and serrated (saw-tooth) pattern of the epithelial crypts. These lesions are significant in the context of colorectal cancer screening and prevention due to their potential for malignant transformation.
Epidemiology
Sessile serrated lesions are more commonly found in the right colon and are believed to account for up to 20% of sporadic colorectal cancers. The prevalence of SSLs increases with age, and they are more commonly identified in women than in men.
Pathophysiology
The pathogenesis of sessile serrated lesions involves genetic and epigenetic changes, including mutations in the BRAF gene and hypermethylation of CpG islands leading to MLH1 silencing. These molecular alterations disrupt normal cell apoptosis and promote unchecked cell proliferation, setting the stage for the development of dysplasia and, eventually, carcinoma.
Clinical Features
SSLs are often asymptomatic and are usually discovered incidentally during colonoscopy. Due to their flat morphology and subtle endoscopic features, they can be challenging to detect and adequately remove.
Diagnosis
The diagnosis of a sessile serrated lesion is primarily made through histological examination of polyp tissue obtained during colonoscopy. Endoscopically, SSLs may appear as slightly elevated, mucus-covered lesions that are difficult to distinguish from the surrounding mucosa. Advanced imaging techniques, such as narrow-band imaging (NBI), can aid in the detection of these lesions.
Management
The management of sessile serrated lesions involves endoscopic removal, typically through polypectomy or endoscopic mucosal resection (EMR). Given the risk of progression to colorectal cancer, it is crucial to ensure complete removal of the lesion. Follow-up surveillance colonoscopy is recommended due to the risk of recurrence and the development of new lesions.
Prevention
Preventive measures for sessile serrated lesions and colorectal cancer include regular screening colonoscopy, lifestyle modifications such as a healthy diet and regular exercise, and possibly the use of aspirin in specific high-risk individuals.
Conclusion
Sessile serrated lesions represent a critical target in the prevention of colorectal cancer. Early detection and removal of these lesions can significantly reduce the risk of progression to cancer. Ongoing research into the molecular pathways involved in the development of SSLs may provide new strategies for prevention and treatment.

-
 Sessile serrated lesion
Sessile serrated lesion -
 Sessile serrated lesion
Sessile serrated lesion -
 Sessile serrated lesion
Sessile serrated lesion -
 Sessile serrated lesion
Sessile serrated lesion




