Acute disseminated encephalomyelitis: Difference between revisions
CSV import |
CSV import |
||
| Line 30: | Line 30: | ||
[[Category:Neurology]] | [[Category:Neurology]] | ||
[[Category:Inflammatory diseases of the central nervous system]] | [[Category:Inflammatory diseases of the central nervous system]] | ||
== Acute disseminated encephalomyelitis == | |||
<gallery> | |||
File:Fulminating_ADEM_showing_many_lesions.png|Fulminating ADEM showing many lesions | |||
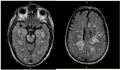
File:Acute_hemorrhagic_Leukoencephalitis_in_a_patient_with_Multiple_sclerosis_(MRI).png|Acute hemorrhagic Leukoencephalitis in a patient with Multiple sclerosis (MRI) | |||
</gallery> | |||
Revision as of 01:23, 18 February 2025
Acute disseminated encephalomyelitis

.png)
Acute disseminated encephalomyelitis (ADEM) is an autoimmune disease marked by a sudden, widespread attack of inflammation in the brain and spinal cord. It is characterized by a brief but intense episode of inflammation in the central nervous system (CNS), often following a viral infection or vaccination.
Pathophysiology
ADEM is believed to be an autoimmune response where the body's immune system mistakenly attacks its own myelin, the protective covering of nerve fibers in the central nervous system. This results in demyelination, which disrupts the normal transmission of nerve impulses. The exact mechanism is not fully understood, but it is thought to involve molecular mimicry, where the immune system confuses myelin with viral antigens.
Clinical Presentation
Patients with ADEM typically present with a rapid onset of neurological symptoms such as headache, fever, nausea, and vomiting. Neurological deficits may include ataxia, hemiparesis, optic neuritis, and altered mental status. In severe cases, seizures and coma may occur.
Diagnosis
The diagnosis of ADEM is primarily clinical, supported by magnetic resonance imaging (MRI) findings. MRI typically shows multiple lesions in the white matter of the brain and spinal cord. These lesions are often bilateral and asymmetrical. Cerebrospinal fluid (CSF) analysis may show elevated protein levels and pleocytosis.
Treatment
The mainstay of treatment for ADEM is high-dose corticosteroids, such as methylprednisolone, to reduce inflammation and immune system activity. In cases where patients do not respond to steroids, intravenous immunoglobulin (IVIG) or plasmapheresis may be considered. Supportive care is also crucial to manage symptoms and prevent complications.
Prognosis
The prognosis for ADEM is generally favorable, with most patients experiencing significant recovery within weeks to months. However, some individuals may have residual neurological deficits. Recurrence is rare, distinguishing ADEM from multiple sclerosis, which is a chronic condition with recurrent episodes.
Related pages
Acute disseminated encephalomyelitis
-
 Fulminating ADEM showing many lesions
Fulminating ADEM showing many lesions -
 Acute hemorrhagic Leukoencephalitis in a patient with Multiple sclerosis (MRI)
Acute hemorrhagic Leukoencephalitis in a patient with Multiple sclerosis (MRI)
