Juvenile active ossifying fibroma: Difference between revisions
CSV import Tags: mobile edit mobile web edit |
CSV import |
||
| Line 24: | Line 24: | ||
[[Category:Pediatric diseases and disorders]] | [[Category:Pediatric diseases and disorders]] | ||
{{Medicine-stub}} | {{Medicine-stub}} | ||
<gallery> | |||
File:A_sagittal_computed_tomography_scan_of_a_juvenile_active_ossifying_fibroma_of_the_frontal_sinus.jpg|Sagittal computed tomography scan of a juvenile active ossifying fibroma of the frontal sinus | |||
File:Hematoxylin_and_eosin_stained_intermediate_magnification_of_a_juvenile_active_ossifying_fibroma.tif|Hematoxylin and eosin stained intermediate magnification of a juvenile active ossifying fibroma | |||
</gallery> | |||
Latest revision as of 01:51, 18 February 2025
Juvenile Active Ossifying Fibroma (JAOF) is a rare, benign, but aggressive fibro-osseous lesion that affects the craniofacial bones. It is characterized by the replacement of normal bone with fibrous tissue and newly formed bone. JAOF predominantly occurs in children and young adults, with a slight male predilection. This condition is notable for its rapid growth and tendency to recur after surgical removal, making early diagnosis and management crucial.
Etiology and Pathogenesis[edit]
The exact cause of Juvenile Active Ossifying Fibroma is not well understood. It is believed to arise from the periodontal ligament, which contains the cell rests of Malassez that have the potential to differentiate into osteoblasts or fibroblasts. Genetic factors may play a role in the development of JAOF, but specific genetic mutations associated with this condition have yet to be identified.
Clinical Presentation[edit]
Patients with JAOF typically present with a painless, expansile mass in the jaw or other craniofacial bones. The lesion can cause displacement of teeth, facial asymmetry, and, in severe cases, visual or auditory disturbances depending on its location. Despite its benign nature, JAOF can be locally aggressive and cause significant morbidity due to its rapid growth and potential to recur.
Diagnosis[edit]
The diagnosis of Juvenile Active Ossifying Fibroma is primarily based on clinical and radiographic findings. Imaging studies, such as computed tomography (CT) scans, are essential for assessing the extent of the lesion and its effect on surrounding structures. Histopathological examination of a biopsy specimen is required to confirm the diagnosis, showing a mixture of fibrous tissue and newly formed bone with varying degrees of cellularity.
Treatment[edit]
The mainstay of treatment for JAOF is surgical excision. Complete removal of the lesion is necessary to minimize the risk of recurrence. In cases where the lesion is extensive or located in a critical area, a more conservative surgical approach may be taken to preserve function and appearance, followed by close monitoring for signs of recurrence. Adjunctive treatments, such as radiation therapy, have been used in some cases but are not commonly recommended due to the risk of malignant transformation and other complications.
Prognosis[edit]
The prognosis for patients with Juvenile Active Ossifying Fibroma is generally good with appropriate treatment. However, the lesion has a high recurrence rate, reported to be between 30% to 58% in various studies. Long-term follow-up is essential to detect and manage recurrences early. The aggressive nature of JAOF and its potential for significant morbidity underscore the importance of early diagnosis and treatment.
See Also[edit]

-
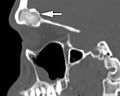 Sagittal computed tomography scan of a juvenile active ossifying fibroma of the frontal sinus
Sagittal computed tomography scan of a juvenile active ossifying fibroma of the frontal sinus -
Hematoxylin and eosin stained intermediate magnification of a juvenile active ossifying fibroma

